SUMMARY: Walking ability is essential for older adults (OAs) to maintain independence and is the…
NEW POSTION STAND ON RESISTANCE EXERCISE PRESCRIPTION FROM ACSM
SUMMARY: The lead recommendation of the new ACSM position stand (PS) is: “our primary recommendation is that healthy adults perform resistance exercise (RE) with ‘high effort’ at least 2x/week, with all major muscle groups being engaged”. Of special interest to older adults (OAs), the PS emphasizes RE is safe for healthy adults of all ages. But the PS also notes that only 10-15% of OAs currently perform RE – even though the benefits can be life-changing – so participation in any manner should be the primary goal for OAs. If you’re past the initial (introductory) stage of RE, the PS says the key performance factor is an intensity of effort that is sufficient to generate positive physiological adaptations: This effort threshold is about 2-3 repetitions-in-reserve from failure (meaning you’re not able to perform another repetition with good form), so “near failure”. To age well, OAs need to develop muscular strength, size & power, as well as balance; and the PS says all these factors improve with RE. However, there are some programming differences needed to best develop each of the physical factors by manipulating training variables like: a) repetition number (assuming high effort); b) weekly RE training volume, which is repetitions grouped into sets of repetitions + days of weekly training; c) loads/resistances used; d) speed of performance or the intention to move as fast as possible. If any of the RE terms are new to you, see my post The Importance of Doing Hard Things and if you have an Instagram account, Dr. Stuart Phillips (who led the PS collaboration) has an outstanding IG post here covering the PS findings.
INTRO
I constantly emphasize that to age well, resistance exercise (1) is THE most important form of exercise for OAs to participate in as the benefits can be truly life-changing. As Tony Boutagy, Ph.D., says, “resistance exercise (RE) may be the most evidence-supported lifestyle intervention we have”. For OAs to successfully participate in RE requires a combination of “big picture” how-to programming principles and individual considerations. This new ACSM Position Stand (PS) can give us confidence in the “big picture” advice.
ACSM is the American College of Sports Medicine, the world’s largest organization of exercise scientists & sports physicians, with over 50,000 members globally. This PS is an “official statement” offering advice for healthy adults to implement RE in the most evidence-supported way. Published this month in ACSM’s official journal, Medicine & Science in Sport & Exercise, this new PS is quite a significant event, as it’s been 17 years since the last ACSM RE PS.
This post is based on three main sources: 1) The ACSM PS document; 2) What other exercise professionals are saying about the PS; and 3) A podcast interview of the lead author, Brad Currier, Ph.D.
Note, this ACSM PS is not expressly targeted for older adults (OAs), so I offer my take as an OA fitness trainer, and will try to distill the PS findings specifically for an OA target audience.
THE ACSM POSITION STAND: OVERVIEW
The full name of the PS is: Resistance Training Prescription for Muscle Function, Hypertrophy, and Physical Performance in Healthy Adults: An Overview of Reviews.
As you might imagine, a lot of research has accumulated in the 17 years since the last PS. The current PS is an “evidence synthesis” built on the data from 137 meta-analyses & systematic reviews with over 30,000 participant subjects (46% women), making it one of the most comprehensive summaries of RE research ever produced.
The comprehensive scope of the PS is extremely significant as that’s what’s required to confidently draw evidence-based actionable conclusions. In contrast, the media (or social media) often report on an single research study in isolation, with no perspective of how it fits in with the totality of evidence on this topic; which might make it interesting, but not nearly enough to confidently draw overall conclusions and useable advice.
THE POSTIVE PHYSICAL, FUNCTIONAL & HEALTH BENEFITS OF RE
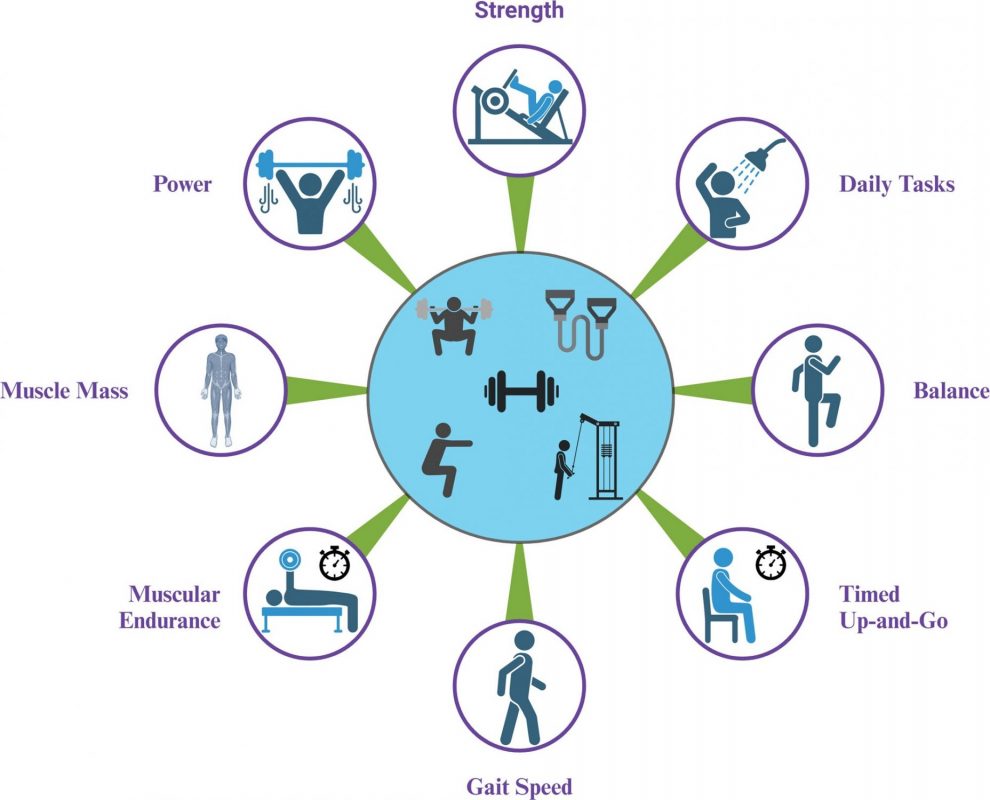
As the title implies, the PS emphasizes that RE training improves multiple physical outcomes. The primary “hallmark” outcomes of RE are:
- Muscular strength (the ability to produce force)
- Muscular size (often termed hypertrophy)
- Physical performance (which is VERY important for OAs)
Physical (functional) performance factors improved by RE include:
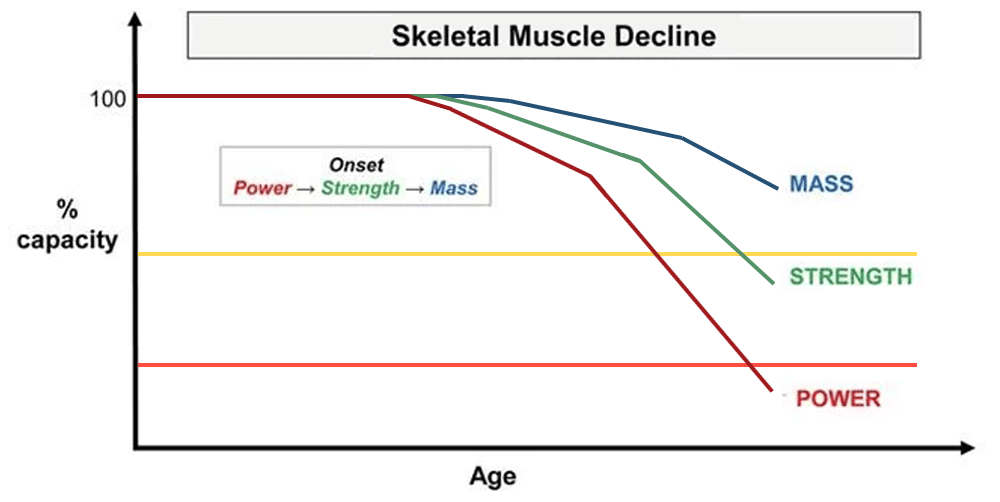
- Power (the ability to move quickly or marry strength with speed)
- Endurance (the ability to produce force for an extended period of time)
- Gait speed (walking speed is a primary indicator of functional ability for OAs)
- Balance (Balance is a primary driver of falls risk for OAs)
- Tests of Multiple Functional Outcomes (sit-to-stand ability; timed up & go)
Additionally, the PS emphasizes the scientific evidence supports that RE improves many health-related outcomes like:
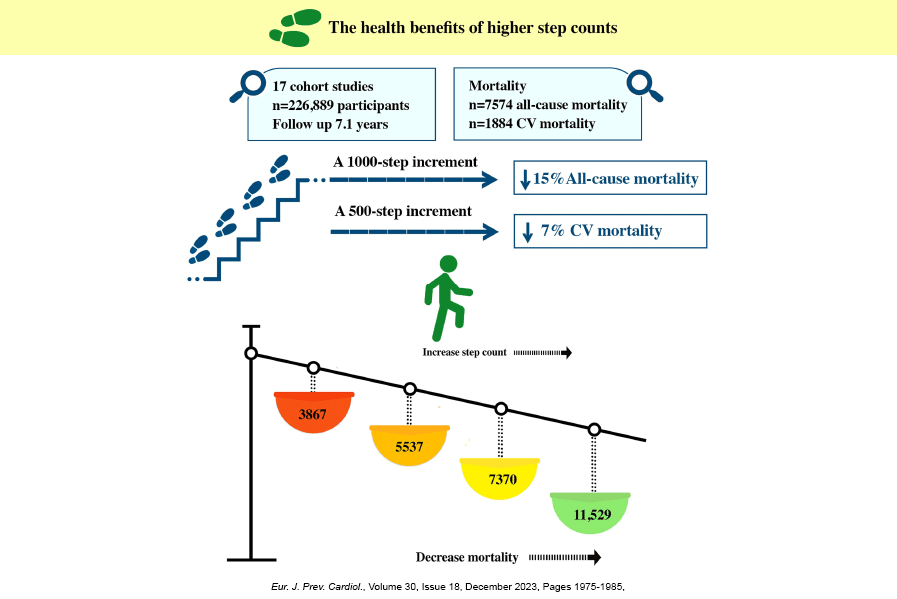
- Reduced all-cause mortality
- Reduced risk of cardiovascular disease (our leading killer)
- Reduced risk of cancer (our number two killer)
- Reduced risk of diabetes (a top-ten cause of death)
- Reduced depression (suicide is a top-ten cause of death)
- Improves sleep quality (especially important for OAs as quality diminishes with age)
RESISTANCE EXERCISE IS SAFE
First and foremost, the PS emphasizes that RE is safe for healthy adults of all ages, including OAs.
Some OA Considerations in Brief
To stay safe, OAs require informed & thoughtful individualized RE programing due to personal physical, medical & functional considerations. For my new clients, much of my job is determining the appropriate starting point for each of the resistance exercise movements, which I call “on ramps”.
In my opinion, OAs benefit from a bit more physical preparation and warmup before engaging in RE compared to younger age groups: depending on individual needs, this could take the form of soft tissue work, joint-tissue mobility work, practicing movement patterns with no resistance, performing lower intensity “practice” sets of RE exercises, or a RE-specific active warmup.
THE MOST IMPORTANT FACTORS FOR SUCCESS: ADHERENCE & EFFORT
The most important factors for positive & beneficial outcomes for OAs are:
- Consistent Participation – AKA Adherence -AKA Showing Up
- Appropriate Intensity of Effort for Each RE Movement
Adherence
The ACSM PS says it’s likely no more than 10-15% of OAs do any RE at all – yikes! – so 85% of OAs aren’t realizing the profound benefits of “the most evidence-supported lifestyle intervention we have”? Yet these are the same OAs who have or will have sarcopenia (under muscled) which will create difficulty when rising from a chair or climbing stairs and contributes to unsteadiness on their feet and an inability to stop a fall if they stumble. These same OAs will find their walking speed decreasing year-by-year and struggle to lift/carry luggage, groceries, or grandkids, not to mention the ultimate physical decline of sliding into physical frailty and dependency.
So, for OAs the best RE program probably isn’t nuts & bolts programing perfection, it’s simply showing up, putting in some effort and being consistent week in and week out with a program that’s been individualized for them– do that and RE adherence will produce the benefits; you could say the RE cake is mostly baked with adherence, and much of everything else is the icing on the cake.
That said, there’s that word “individualized” above; OAs do require more attention to the most appropriate and accessible RE exercises (and modifications of those exercises) due to personal physical, medical & functional considerations – and attention to reasonably clean exercise technique is important too as it’s not advisable to just “slop” through your RE workout. So, when in the process of “just showing up”, you have to be able to perform your program reasonably well, so some care and individualized attention is quite helpful & important.
Intensity of Effort
The ACSM PS emphasizes you have broad latitude for the particular RE (1) resistance tools and methods you use or the load/resistance/weight you use (which dictates how many repetitions you’re able to perform). Anywhere you train (home or gym), most resistance tools & methods work and a range of repetitions from 5 to 30 will work, as long as the effort/intensity level is enough to stimulate a positive physiological adaptation and you accumulate enough volume of RE (sets of repetitions plus days you train per week).
What’s “enough” effort/intensity? The PS states this threshold of effort/intensity is about 2-3 repetitions-in-reserve (RIR) before you can’t do another repetition in good form, so “near failure”. In my post The Importance of Doing Hard Things, I discuss this concept and others in more detail.
What’s “enough” volume of RE? At least one set of 6-8 RE exercises performed 2X/week, but 2 sets of each exercise is clearly better if you have the time & energy.
WHAT ELSE IS IMPORTANT TO KNOW
“Starting is not the hardest part, staying is”
In the podcast, Dr. Currier emphasizes that almost 50% who start RE drop out, and 2/3 of the dropouts happen within the first 1-2 months. So, finding a reason to keep coming back and getting the help you need to develop an individualized program you can stick with are key.
The best news: if you’re an OA new to RE, any RE training is going to produce positive gains
When first starting RE even “minimal-dose”, less than optimal intensity training, can produce meaningful gains in strength & power! So, just get started and build some positive momentum, confidence and RE skill/familiarity.
Older adults should prioritize lower body RE training
With OAs, your lower body are your “wheels” and anti-gravity muscles which make it possible to rise from a chair, climb/descend stairs, and walk to get around and do what you want in life. Your lower body also contains the largest muscle groups in your body, so this is where you need to prioritize RE to prevent sarcopenia (being under muscled).
Examples of key lower body movement patterns are:
- Sit-to-stands (blog post here)
- Squats
- Step Up/Lower Down
- Split Squats
- Dead Lifts
- Dynamic back bridges (hip lifts, glute bridges)
- Heel Raises
Priority movement patterns (exercises) performed first in your RE workout
For OAs, this means lower body as per above.
Move through as big a range of motion as you are safely able
For many OAs, range of motion needs to be modified for various reasons, but do what you can safely: descend on a squat as low as you can control & stabilize; perform sit-to-stands from as low a chair as you are able to overcome gravity from; perform a Step Up/Lower Down from as high a step as you are able to overcome gravity & control the descent; for heel raises, when you can perform them well from the ground, move your forefoot onto a platform (deficit) so you can get a greater range of motion.
Perform at least 2 sets of repetitions of each exercise if you have the time & energy
The PS states “Healthy adults are advised to complete at least 2 sets/exercise”, and I think this is generally good advice for OAs, if you have the time & energy as it will produce greater positive results than 1 set/exercise. If your main goal is gaining muscle mass (hypertrophy), then it’s possible even more than 2 sets/exercise would be helpful, as the PS emphasizes that hypertrophy is exercise-volume dependent, but then adequate recovery could become a factor depending on how many times per week you wish to train.
GENERALIZED BIG PICTURE RE PROGRAMING FOR OAS
“All major muscle groups” or total body programing at its simplest might look like this:
- Lower body
- Upper body push
- Upper body pull
- Core (midsection-trunk of body)
- Loaded Carries
If lacking time or energy or motivation, you can omit any of the categories except lower body, which is non-negotiable for OAs.
Primary Emphasis: Strength
-Relatively heavier loads/resistances which dictates lower repetition ranges, perhaps 5-10 for OAs; PS says 80% or greater for your one-repetition maximum, which is about 8-9 repetitions
-Full range of motion as safely possible
-Lower body first as primary strength goal for OAs and most demanding exercises
Primary Emphasis: Hypertrophy
-Any load/resistances that allows for 5 to 30 repetitions, as long as effort is close to failure
-Emphasize the part of the movement that slows you or the resistance down from gravity’s effect, which is called the eccentric muscle contraction (descent on standing lower body exercises); which means emphasize slower eccentric control, which takes concentration & discipline as the temptation is to move through that portion of lift as fast as possible, i.e., drop down rather than lower down under control
-Higher volume, which means more sets per week per movement pattern or muscle group or body part or region (like lower body); PS stand says 10+ sets per body part or muscle group per week
Primary Emphasis: Power
-Lower loads/resistances
-Intent to go as fast as possible on the part of the movement accelerating against gravity (ascent on sit-to-stands or squats) which is called the concentric muscle contraction. Descent is always performed slowly.
-Relatively lower volume and repetitions (3-8 repetitions per set as you want to keep speed high and not have it drop off with too many repetitions)
-For OAs, most accessible power development exercises are first high-speed sit-to-stands, and when those are mastered, try high speed concentric portion squats (descent or lowering always slow)
Footnotes:
(1) Resistance exercise, also referred to as resistance training or strength/weight training, is a form of exercise where muscles are exercised by contracting against an external resistance (often called the load) supplied by tools like dumbbells, barbells, kettlebells, pin-selected weight stack machines, short or long resistance bands, water, or in some cases just body weight, while attempting to progressively increase the challenge over time to improve muscular strength (ability to generate force), hypertrophy (increased muscle size) and power (ability to move more quickly).
Related Posts