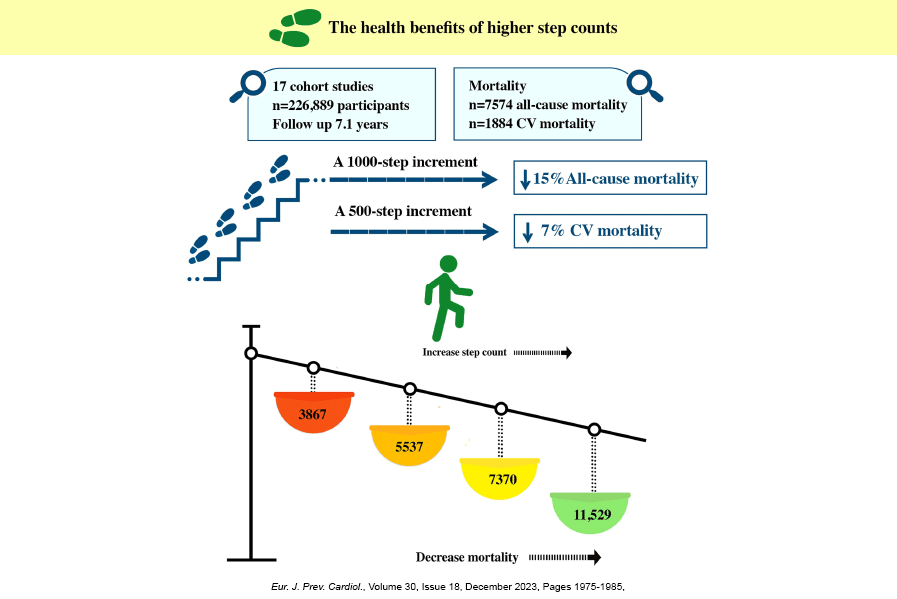
SUMMARY: Walking ability is essential for older adults (OAs) to maintain independence and is the…
THE NUMBER ONE RULE OF OLDER ADULT FITNESS
SUMMARY: To age well, older adults (OAs) must optimize for physical function and minimize their chronic disease risk. It’s very important for OAs to know what they’re up against with the physical/functional decline with aging, so this post is about some big-picture factors involved in optimizing for physical function which I’ve organized around two essential rules of OA fitness, as well as some characteristics of aging muscle tissue and the predictable functional decline that happens with aging. We cover essential concepts of functional aging like: a) functional thresholds of aging; b) functional reserve capacity; c) favorable & unfavorable responses of muscle tissue due to exercise or disuse; e) disuse events and new insights into their contribution to functional decline; f) OAs incomplete physical recovery from disuse events; and g) tips to help avoid & minimize disuse events to help maintain your physical function.
INTRO
Our physical performance declines with aging. What we can do about it? This is not really on most older adults (OA) radar, except when it’s too late. It should merit some attention, though, because OAs don’t randomly become physically incapable; the process starts in middle age and we know the functional decline with aging has specific causative factors that are modifiable. In fact, provided we make the correct informed choices, we have a lot of control over our functional decline trajectory. “Informed choices” is key since aging well starts with this principle: OAs must strive to optimize for their physical function and concurrently seek to minimize their chronic disease risk.
It’s very important for OAs to know what they’re up against with aging’s functional decline, so this post is about some key big-picture factors associated with “optimizing for physical function”, as OAs need to aware of these factors to make the most informed choices. I’m organizing this discussion around two essential rules of OA fitness (Rule #0 & Rule #1), as well as some characteristics of aging muscle tissue and the predictable functional decline that happens with aging.
Rule #0 is foundational because it’s about adherence: to optimize for physical function you absolutely must regularly participate in exercise/fitness activities – specifically aerobic (1), resistance (2), and balance exercise (3). But regular participation is a tough nut to crack for the majority of OAs, since according to a new American College of Sports Medicine Position Stand, it’s likely no more than 10-15% of OAs meet the complete exercise guidelines; and OAs are particularly lacking for resistance exercise (4) which is crucial to stave off physical declines. So, it can’t be overstated: it’s imperative to nail down Rule #0 no matter what – have a personal reason(s) that motivate you, get the help you need to implement exercise effectively, and build systems into your life to make physical activity a habit you can’t live without.
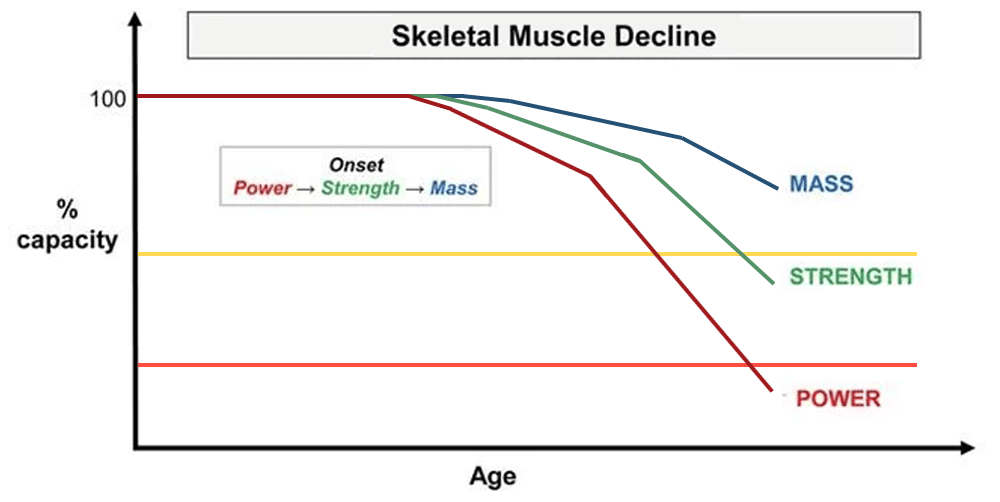
Rule #1 relates to situations to avoid if OAs are to minimize & delay the physical decline represented in the headline image above – “minimize & delay” means keeping the above functional aging curves as flat/horizontal for as long as possible. OAs accomplish this “flattening” by nurturing accelerators of functional capacity – regular exercise (Rule #0) – and avoiding accelerators of functional decline which, based on fairly new information, are what are termed “disuse events” (Rule #1).
The above headline image is a graphical representation of the predictable physical/functional decline with aging – and it’s all one direction – downward. But the good news is the downward rate of these physical/functional capacity slopes (the trajectory) is quite variable, depending on how well you can follow the Rules (#0 & #1).
Most any domain of functional aging or physical performance would plot out the same way, including super important domains for OAs like aerobic capacity and dynamic balance. I’ve discussed aerobic capacity and dynamic balance in multiple previous posts here, here, and here.
Please note – This is post is inspired by, and draws from, the following sources:
* Muscle Disuse as a Pivotal Problem in Sarcopenia-Related Muscle Loss and Dysfunction
* The Impact of Step Reduction on Muscle Health in Aging: Protein & Exercise as Countermeasures
* Sarcopenia: What it is, Symptoms, and How to Prevent It
THE FUNCTIONAL THRESHOLDS OF AGING
“Functional thresholds” are inflection points of functional aging that have real-life negative consequences for OAs.
THE FUN THRESHOLD: Look at the title image above and move your attention part-way down the graph to the yellow horizontal line across the slopes for muscle mass, strength (5) and power (6) – this yellow line is the “fun” threshold of functional aging – the point at which your physical/functional decline forces you to modify or avoid your (fun/satisfying/vital) activities. We’d like to delay crossing this line as long as possible to maintain the most enjoyable, vital and, yes, fun quality of life.
DISABILITY THRESHOLD: Now, draw your attention to the red horizontal line below the “fun” threshold. This red line would be your disability threshold – the point where you lose your independence because essential activities of daily living are impossible for you without help from others. Once you reach the disability threshold, it’s likely you might be frail or pre-frail (7) and/or perhaps relocated to an assisted living facility. Every OA would like to delay & avoid this threshold point for as long as possible.
FUNCTIONAL RESERVE CAPACITY
Functional reserve capacity (also called physiologic reserve) is the difference between an OA’s current functional capacity and the functional thresholds discussed above. The smaller your functional/physiologic buffer is between your current physical capabilities and the disability threshold, the closer you are to dependence, debilitation, and frailty.
Functional reserve capacity is a significant factor in your ability to perform daily activities with ease or with extreme difficulty or not at all. If you have no “gas left in the tank” for an activity you are maxing out physically. In the realm of muscular strength expression, this is called “one-rep max living” from the resistance exercise term “one-rep max”, which is the maximum amount of weight you can lift for one repetition. Imagine your sit-to-stand (rise from a chair) one-rep max is less than your body weight; this means you require assistance to get out of a chair every single time.
Note, also, that without a significant functional reserve capacity, you have literally no physical resilience (your ability to bounce back from life’s demands, circumstances, or situations). With no physical resilience, any stressor that comes along like injury or illness will push you further into physical decline or actual debilitation – and this relates directly to OA fitness Rule #1 discussed below about avoiding “disuse events” at all cost.
MUSCLE RESPONDS TO THE DEMANDS YOU GIVE THEM (OR DON’T)
Muscle tissue contracts to generate forces which pull on bones to overcome gravity and create movement and stability – and muscles are really good at this, if they stay in practice; meaning muscles respond & adapt to the physical demands you give them (or don’t give them). A cornerstone concept of physical/functional aging is this: Aging muscle is extremely sensitive to regular contractions from physical loading and movement – it’s not an exaggeration to say aging muscles “crave” this loading challenge to stay vital, healthy & functional. Keep muscles contracting regularly with the right physical stimulus and you can stave off the steep declines of the functional curves in the title image above, but allow muscles to remain inactive and bad things happen to muscle mass, as well as muscle quality & performance. Lack of regular muscular contractions has negative metabolic consequences as well – blood sugar (glucose) goes up, inflammatory compounds increase and fat can literally infiltrate the functional machinery of muscle and impair its ability to contract effectively.
DISUSE EVENTS
The slopes in the title image above make it look like there is a smooth, gradual, predictable decline of functional aging, which may be a reasonably representation of what happens when you zoom out and plot the functional changes at the population level. But relatively new research shows something different when you consider an individual OA involved in real-life aging, as the decline can happen in a series of step-wise reductions as shown in the red-colored “punctuated decline” line in the schematic graph below.
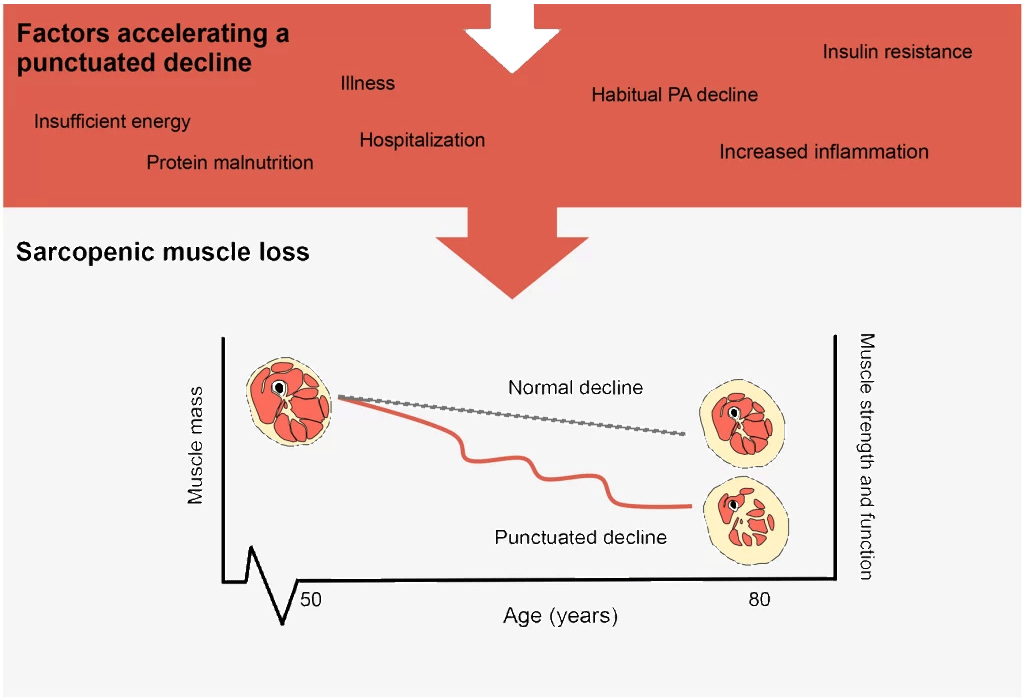
And this is where this new research gets really interesting: These step-wise reductions in physical capacity/function are caused by specific situations of non-activity which researchers term “disuse events”. Disuse events create significant & measurable reductions in muscle mass, strength, speed, balance, and other functional impairments; and can also create increases in visceral fat (8) and systemic inflammation and cause other metabolic dysfunctions like insulin insensitivity & elevated blood glucose.
Specific categories of disuse events might be:
1) bodily injuries
2) limb immobilization from joint replacements or bone breaks from falls
3) situations of bed rest, hospitalization or surgery
4) viral/bacterial illness events like pneumonia, Covid, influenzas, RSV or shingles
5) incredibly, even seemingly benign events like reducing how much you regularly walk (reduced daily step count) can create measurable functional and metabolic impairments
INCOMPLETE RECOVERY FROM DISUSE EVENTS FOR OLDER ADULTS
For OAs, it turns out disuse events are accelerators of functional decline over and above the “normal” declines expected due to chronological aging itself – and this is a relatively new insight into the causes of functional decline with aging. OAs can experience a disuse event and never recover the full physical capabilities they had before the disuse event. Factors that may contribute to this lack of physical resilience after a disuse event might include:
1) Many OAs are mostly sedentary, so they’re already starting with a body that’s detrained due to habitual sedentary behavior, that’s their baseline muscular environment.
2) Even before a disuse event, OAs start at a significantly lower functional level than younger adults, so OAs have less functional reserve and can’t afford to give away much more as they are closer to the disability threshold discussed above.
3) Research shows OAs have a hard time physically bouncing back from a disuse event; it may take a significant amount of time and specific physical training to restore the functional capacity they had before a disuse event. Absent specific physical training, a disuse event can put OAs at a lower physical baseline post disuse event than before – they’ll experience a new functional normal which is lower than before – and this scenario can, and perhaps will, happen repeatedly throughout an OA’s life.
THE NUMBER ONE RULE OF OA FITNESS
So, not surprisingly, the number one rule of OA fitness is this: AVOID DISUSE EVENTS AT ALL COSTS.
This Rule #1 is often expressed in statements like: “don’t get injured”; “stay in the game”; “consistency beats intensity”.
What are some best practices for following OA fitness Rule #1?
1) Bodily injuries
*Work on your balance, strength & power as falls are a big contributor to injuries and broken bones
*Use good movement strategies, movement aids, vision enhancing eye wear, and lighting to negotiate your surroundings – and use good judgement and never move carelessly
* You have a choice for how your home environment is organized – avoid clutter, throw rugs and other tripping hazards
*Use extreme caution when descending stairs and hold onto hand rails
*Work on your joint-tissue mobility as stiff joints & tissues can contribute to injuries during physical activity or exercise – toe extension, ankle dorsiflexion, hip flexion/extension, thoracic spine rotation and overhead shoulder flexion are OA mobility essentials
*OAs require more physical preparation before exercise: Preparation strategies could include general warmup, general movement preparation, joint-tissue mobility work and movement pattern practice before loading
*Abruptly increasing frequency, intensity, duration, and especially volume of exercise is a well-known risk factor for exercise injuries – make sure to progress or advance very gradually
2) Limb immobilization
*Work on balance, strength & power as falls are a big causative factor for broken bones
*Osteoarthritis is not a “wear & tear disease”, it’s mostly a biological process driven by inflammation, metabolic dysfunction, and impaired tissue repair, so work to optimize visceral fat levels, blood glucose, systemic inflammation (eat a plant-based diet), and recovery/restorative methods like sleep
*Resistance exercise is essential for best osteoarthritis management
*If a joint replacement is inevitable, do “pre-habilitation” physical training before surgery to enhance recovery and minimize time spent in a disuse event
3) Bed rest
*Be in good physical condition before situations of bed rest, hospitalization or surgery
*Make sure you’re getting optimal amounts of protein before and after surgeries as you may require more than normal
*Research shows that any loading or muscular challenges while in bed rest can help preserve some muscle quality & function
4) Viral/Bacterial illness
*Use vaccines as they reduce severity of all the common illnesses that OAs are in high-risk category for serious complications; like bacterial pneumonia, Covid, influenzas, RSV, and shingles
*Vaccines reduce other serious complications from viral/bacterial illnesses like heart attacks and strokes that are more likely to occur; vaccines also decrease overall mortality risk
*Wear well-fitting masks – particularly in crowed indoor locations & planes or locations where sick people are likely to frequent (like doctor’s offices, hospitals, pharmacies) – they aren’t protective for the wearer if they’re worn loosely as there is no barrier to outside air
*Wash/sanitize hands often and never touch eyes, nose or mouth with un-sanitized fingers
*Get adequate sleep
*Follow a largely plant-based eating pattern which minimizes ultra-processed foods
5) Reduced daily step counts
*Walk, walk, walk; if you have to reduce for any reason, make the reduction as minimal as possible for the least number of days and least cumulative daily amount
*If your walking endurance is compromised, break walks into doable small amounts that fit your current capacity and do as many each day as you can
*To minimize walking-related injuries and improve walking ability, work on your joint-tissue mobility for toe extension, ankle dorsiflexion and hip flexion/extension
*Work on toe, foot, lower leg and hip strength for walking power and minimizing walking-related injuries
*Use walking aids like canes and Trekking poles if you need them for safety
*Shoes are a big & important topic: laced securely please, and big-as-a-boat walking shoes are probably not doing you any favors, regardless of current trends
Footnotes:
(1) Aerobic exercise is also called cardiorespiratory exercise or cardiovascular exercise or even “cardio” for short. Cardio usually involves larger muscle groups used in a rhythmic & somewhat continuous manner.
(2) Resistance exercise is also called weight training or strength training. The “resistance” to movement can come from elastic bands, cords, dumbbells, barbells, kettlebells, cable/pulley apparatus, or pin-selected weight stack machines and, sometimes, body weight. The “resistance” is often called a “load”.
(3) Balance is the ability to maintain your center-of-gravity over your base of support (most often your feet). Dynamic balance is the most important for OAs to enhance and maintain as they age.
(4) So, 85% of OAs aren’t realizing the profound benefits of “the most evidence-supported lifestyle intervention we have”. Yet these are the same OAs who have or will have sarcopenia (under muscled, lacking strength & power) which will create difficulty when rising from a chair or climbing stairs and contributes to unsteadiness on their feet and an inability to stop a fall if they stumble. These same OAs will find their walking speed decreasing year-by-year and struggle to lift/carry luggage, groceries, or grandkids, not to mention the ultimate physical decline of sliding into physical frailty and dependency.
(5) Muscle strength is the ability to generate force to move or accelerate loads or limbs.
(6) Power is the ability to combine strength with speed of movement. For OAs, practical application is the ability to move your legs quickly, particularly in situations where you need to be able to move your base-of-support (feet) back under your center-of-gravity in order to stay balanced to prevent a fall.
(7) See Fried’s Frailty Index
(8) This is fat deposited in & around the internal organs. Also called central fat or intra-abdominal fat. Visceral fat is a health risk and increases systemic inflammation as well as risk for heart & blood vessel disease and diabetes and perhaps even cancer.
Related Posts