SUMMARY: Walking ability is essential for older adults (OAs) to maintain independence and is the…
THE IMPORTANCE OF DOING EASY THINGS: WALKING EDITION
SUMMARY: The most effective strategy to combat physical aging is to bring some intensity & challenge (hard things) to your exercise/physical activity. But many older adults (OAs) can’t always challenge themselves with “hard things”. Thankfully science tells us that basic physical activities (PA) like walking (easy things) can help with health and aging too. “Easy things” won’t capture the same magnitude of physical/health benefits as “hard things”, but the benefits are there. Walking has a consistent body of research which implies that every step counts toward improving health and lowering our risk of death. Below, I discuss the three most recent meta-analyses which examine daily walking step counts and subsequent risk of death & disease. All three meta-analyses point in the same positive direction: The more steps you take, the longer & healthier you’re likely to live – and the benefits start at amazingly low daily step counts – and most encouragingly, the biggest proportional health & mortality benefits come at the lower end of daily step counts, which should be doable for almost all OAs.
INTRO
Read my series of posts on “The Importance of Doing Hard Things” and you’ll think I’m all about bringing intensity & challenge (hard things) to your exercise/physical activity. Yes, I certainly am, because that’s the most effective strategy to combat physical aging. But we don’t live in a perfect world. Many older adults (OAs) can’t always challenge themselves with “hard things” (1) for a variety of reasons, but thankfully science supports the idea that basic, and relatively easy, physical activities can help with health and aging too. The key seems to be just getting out of the sedentary lifestyle category, so let’s see what it takes…
For OAs, physical aging is accelerated when we’re physically inactive – a sedentary lifestyle – and sadly this is the default for many OAs. Conversely, to optimally slow down the physical effects of aging, OAs should have a dual-intensity physical activity plan: a physical activity “floor” (lower effort limit) of easier things which is alternated with a physical activity “ceiling” (upper effort limit) of harder things.
If you’ve got both floor & ceiling physical activities (PAs) in place, the easy things can help your body to recover from the hard things while still providing some intrinsic health & anti-aging value on their own. But let’s be clear: Bottom line, OAs need “something” in the realm of regular PA; so that’s where floor-type PAs may come in – as an absolute minimum level of PA for those who can’t or won’t do more. With floor PAs alone, you won’t capture the same magnitude of physical or health benefits as ceiling activities, but you WILL get some benefits!
Walking is the primordial PA, so OAs should consider a certain amount of walking as the rock bottom PA floor. And the great news about walking is the compelling and consistent body of research which tells us that every step counts toward improving our health, aging capability, and lowering our risk of death.
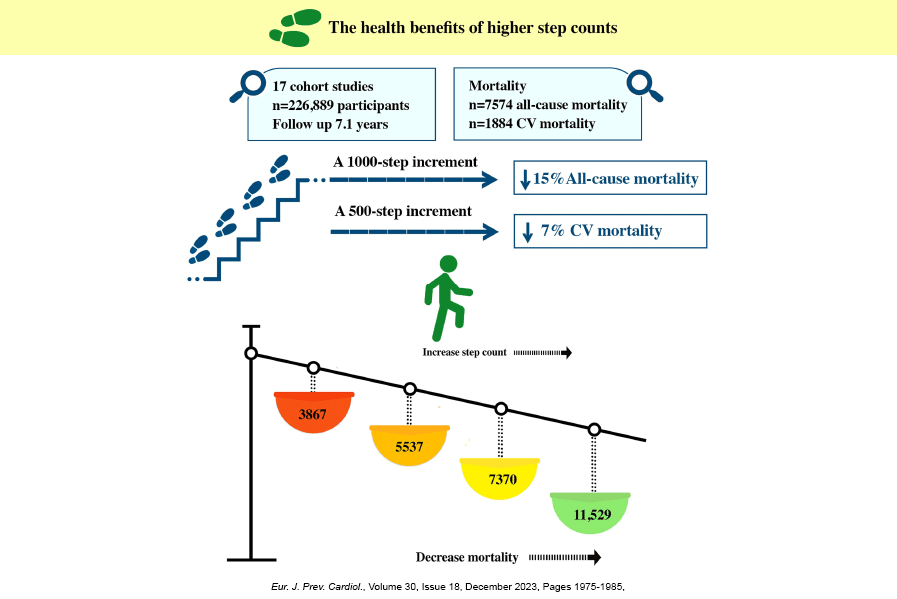
Below, I discuss three very recent, large-participant meta-analyses (2), that examine daily walking step counts and subsequent risk of death and chronic diseases. All three meta-analyses point in the same very positive direction: The more steps you take, the longer & healthier you’re likely to live – and the benefits start at a surprising low daily step count (especially for OAs). Look at the title image above which comes directly from one of the meta-analyses – every increase of 1K-step increment decreases all-cause mortality by 15% and every increase of 500-step increment decreases cardiovascular mortality 7%.
DAILY STEP COUNTS AND RISK OF DEATH & DISEASE: OVERVIEW
“The message that every step counts…should be emphasized as a core public health message…” Dr. Ding Ding, author of one of the meta-analyses discussed below
This field of study is fairly young, starting in 2014 according to Dr. Ding, and the three meta-analyses I cover below include all the highest quality studies since then. The studies included in the meta-analyses all have the same format: Assess device-measured daily step counts for a period of time at the outset, and then follow participants for a period of time (measured in years), and then quantify the association between daily steps and risk of death and disease, while attempting to statistically adjust for as many confounding factors as possible that might skew the results. To help ensure accurate findings, the authors of the meta-analyses also used methods like excluding participant deaths in first two years of follow up to minimize potential for “reverse causation”, and an interesting “leave one out analysis”, which excludes one study at a time from the results to ensure that one large study, or a study with extreme results, doesn’t skew the meta-analysis findings.
MAIN OVERALL FINDING: The studies detail a very compelling inverse relationship between daily step counts and the risk of death from all causes (all-cause mortality) as well as chronic diseases of aging like atherosclerotic cardiovascular disease (ASCVD), our number one cause of death.
MAIN OVER-ALL USEFUL CONCLUSIONS:
1) There is a point of diminishing health returns, or an inflection point, where walking more (higher daily steps) may provide a little bit more benefit, but the health returns for the time & effort diminish substantially.
2) OAs need less steps per day to reach the diminishing health returns inflection point than younger adults – this is great news for OAs!
3) Health & mortality benefits can start at amazingly low daily step counts – just 3K to 4K steps/day – approximately 1.2 to 2 miles.
4) The biggest proportional health & mortality benefit seems to come at the lower end of daily step counts – meaning if you’re at 2K daily steps today, getting to 4K matters more than someone at 8K getting to 10K.
5) Relatively small incremental increases in daily step counts create a health & mortality benefit signal measured by these meta-analyses – each increase of only 1K steps/day for all-cause mortality and, amazingly, only 500 steps/day for ASCVD have measurable effects!
DAILY STEP COUNT META-ANALYSES STUDIES
The three most recent meta-analyses which study the relationship between daily step counts and the risk of death & disease are authored by Drs. Amanda Paluch, Maciej Banach, and Ding Ding, and we briefly review each below.
DR. PALUCH’S 2022 META-ANALYSIS included 15 studies with 47,471 participants (68% female) with average age of 65 and an average follow up of 7.1 years. An interesting aspect of this meta-analysis is it included non-published studies – this is relevant because published studies are much more likely to contain positive results (termed publication bias), while unpublished studies are not.
Key findings:
1. The daily step target for most efficient mortality risk reduction depends on your age.
2. Adults age 60 and up reached the point of diminishing returns for all-cause mortality at 6-8K steps/day.
3. Adults aged less than 60 reached the point of diminishing returns for all-cause mortality at 8-10k steps/day.
DR. BANACH’S 2023 META-ANALYSIS included 17 studies with 226,889 participants (49% male) with an average age of 64 and an average follow up of 7.1 years. An interesting aspect of this meta-analysis is they quantified daily step counts up to 20K steps/day.
Key findings:
1. All-cause mortality benefits started at a floor of only 3,867 steps/day.
2. Cardiovascular mortality benefits started at a floor of only 2,237 steps/day.
3. For each 1K-step increase above floor steps/day (3,867) there was a 15% decreased risk of all-cause mortality.
4. For each 500-step increase above floor steps/day (2,237) there was a 7% decreased risk of cardiovascular disease death.
5. There was a 48% reduction in all-cause mortality at just 5,500 steps/day.
DR. DING’S 2025 META-ANALYSIS included 31 studies from 24 participant cohort groups and is the “largest and most comprehensive synthesis of the association between daily steps and major health outcomes to date”. A key aspect of this meta-analysis is it followed a diverse range of health outcomes besides all-cause or cardiovascular mortality.
Key findings:
1. Health and mortality benefits started when step counts got above 2,000 steps/day!
2. 4K steps/day resulted in substantial 36% all-cause mortality risk reduction compared to 2K steps/day.
3. Much of the health & mortality benefits could be captured at 7K steps/day.
4. Much of the cardiovascular disease incidence benefits could be captured at 5,386 steps/day.
5. Although the incremental protection beyond 7K steps/day was small, “health risks generally continued to decrease with every 1K/day increase in steps across most outcomes up to 12K steps/day”.
DOES WALKING FASTER INCREASE HEALTH & MORTALITY BENEFITS?
My personal bias is that adding intensity (walking faster; higher walking “cadence”) will provide added health & mortality risk reduction (3), but proving it with these studies was a challenge. Dr. Paluch and Dr. Ding looked at this question and did find evidence to support that walking faster is better, BUT the evidence was NOT completely consistent or conclusive – perhaps due to what Dr. Paluch explains below:
“Disentangling the health associations of stepping rates from step volume in daily life is difficult because individuals who walk at a faster pace usually accumulate more steps per day than those who walk at a slower pace”.
If you statistically adjust for total step daily counts to account for the above, Dr. Ding found:
1. An inverse linear association between peak-30-minute step cadence (highest number of steps accumulated over a 30-minute time interval) and all-cause mortality which was significant.
2. But mixed evidence for cadence and other health outcomes.
Dr. Paluch looked at this question several different ways by calculating; a) peak 30-minute and peak 60-minute step rates; and b) minutes of time spent walking at 40 steps/minute and 100 steps/minute.
Dr. Paluch’s findings:
1. Higher stepping rates were associated with lower risk of mortality without adjusting for total steps per day.
2. The association between peak 30-minute and peak 60-minute step rates and all-cause mortality risk reduction remained significant after adjusting for steps per day.
3. After adjusting for total step/day volume, time spent walking at 40 steps/minute and 100 steps/minute were not associated with all-cause mortality risk reduction, except in one subgroup of results at 100 steps/minute.
Footnotes:
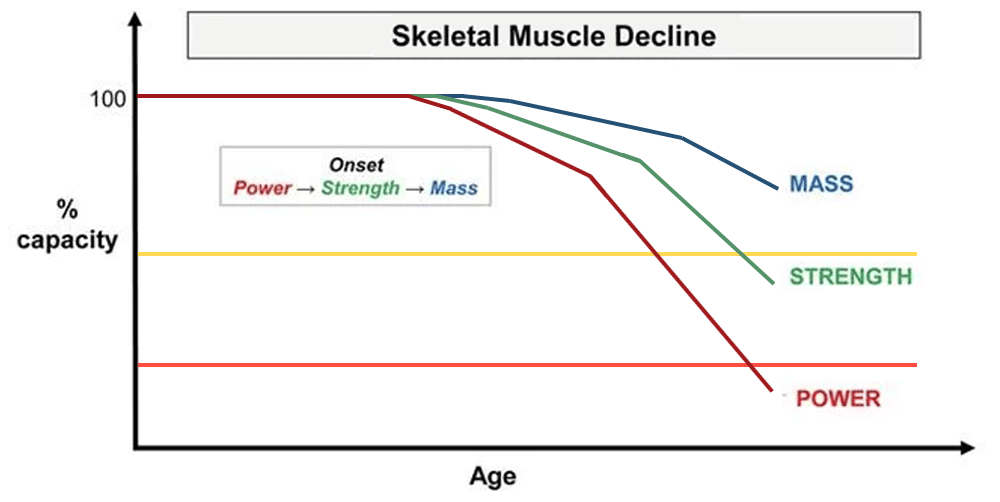
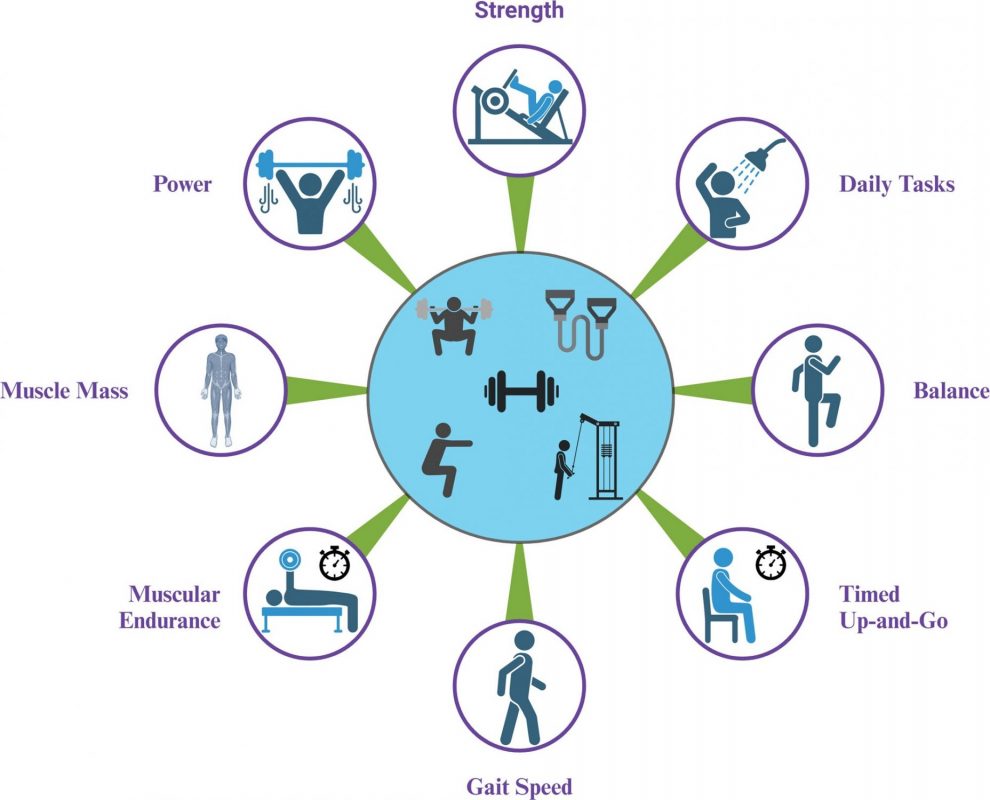
(1) The most important “hard thing” for OAs to include is resistance exercise as it has the power to be functional transformative while most effectively staving off the negative physical effects of aging.
(2) A meta-analysis is a study of studies which synthesizes the results of multiple studies which address the same question to produce a more reliable conclusion than any single study.
(3) Some research points to faster walking speeds as a falls risk for some OAs, so that’s why I generally advocate for walking uphill to add intensity & physical challenge instead of walking faster. Some research also seems to suggest that we quickly adapt & become more efficient to faster walking cadences, which will decrease the relative challenge or intensity.
Related Posts